


“Children are the world’s most valuable resource and its best hope for the future.”
— President John F. Kennedy (July 25, 1963)
No line better captures the urgency for investing in children. When we measure our country’s promise this way, we are forced to ask: do our nation’s policies measure up to doing right by our nation’s children and our future.
Earlier this week, Department of Health and Human Services (HHS) Secretary Robert F. Kennedy released his “Make Our Children Healthy Again” strategy. How does it measure up?
From the outset, the Make America Healthy Again (MAHA) report disappoints and reads like performance art: brief touches on various topics that are filled with meaningless words that are woefully short of strategy and progress.
Marion Nestle, a renowned nutritionist and professor at New York University, noted that the report is heavy on intentions but little else. According to Nestle:
Everything else is waffle words: explore, coordinate, partner, prioritize, develop, or work toward.

Tragically, the performative words seek to obscure a hollow framework: one that undermines trust in public health institutions, shifts focus from proven programs to ideological reinterpretation, distracts from real investment in children’s well-being, and fails to achieve the previously stated purposes, which is to make children healthy and protect children from harm, including nicotine and toxic pesticides.


In sharp contrast, earlier this year First Focus on Children submitted to Secretary Kennedy a report, which was built on evidence-based and real-world solutions from experts and the child advocacy community. Our blueprint centered on:
Strengthening Medicaid and the Children’s Health Insurance Program (CHIP) to guarantee access to pediatric care.
Protecting vaccines, the Centers for Disease Control and Prevention (CDC), and other public health institutions and programs from erosion.
Expanding maternal and child health infrastructure to combat infant and maternal mortality.
Addressing the children’s mental health crisis that is threatening the health, well-being, and lives of kids.
Closing racial, geographic, and socioeconomic gaps in child health outcomes through data-driven strategies and community support.
Improving pediatric readiness in emergency care for children to improve health care outcomes and to save lives.
Balancing the rights and protections for adolescent health and well-being.
Expanding tobacco control to protect America’s youth from harm.
Protecting the health and well-being of ALL children, including immigrant children.
Reducing child abuse and neglect by expanding prevention, addressing inequities, and improving services and care.
Cutting child poverty, as it is a key social determinant of health and well-being for children.
Improving and protecting health care services in other settings, including Head Start, child care, and schools.
Increasing gun safety, as firearms are the leading cause of death of children ages 1-17.
Investing in pediatric research through sustained funding at the National Institute for Child Health Development (NICHD) at the National Institutes of Health (NIH), including strategies to cure pediatric cancer.
This isn’t just a difference in approach: it’s a immense difference in values and legacy.
Measured by President Kennedy’s quote, the federal MAHA strategy falls tragically short, as it does not even positively address a single one of these 14 priorities. Instead, what Secretary Kennedy offers is skepticism where we need trust, rhetoric rather than investment, ideology where we need science.
What children need is a genuinely child-focused agenda rooted in health coverage, public health, medical research, science, equity, and evidence – not cuts to their health care and coverage.
The MAHA Plan: Undermining Children’s Health Coverage
“We can say with some assurance that, although children may be the victims of fate, they will not be the victims of our neglect.” - President John F. Kennedy (Oct. 24, 1963)
The most striking thing about the federal MAHA strategy isn’t what it says: it’s what it neglects or leaves out. For all its language about wellness, longevity, and future generations, the strategy fails to support the very systems that make children healthy in the first place.
In sharp contrast, the 14-point blueprint cited above lays out a clear path forward: build on the tools we already know work, backed by data, clinical experience, and family needs. That means protecting and expanding core programs like Medicaid, CHIP, WIC, and maternal and child health services. It means investing in pediatric research, defending the vaccine infrastructure, strengthening public health institutions, and directly addressing the inequities that drive disparities in outcomes.
These aren’t theoretical policy ideas: Medicaid and CHIP are life-saving initiatives, especially for low-income children, children with disabilities, children in rural areas, foster kids, and children of color. Medicaid and CHIP are the real-world mechanisms through which 37 million children – nearly half of all U.S. children – receive preventive care, immunizations, screenings, and treatment. These programs save lives, reduce disparities, and promote better outcomes from infancy to adolescence.
Medicaid and CHIP saves lives by improving access to care, reducing preventable deaths, and promoting better health outcomes for children.
Unfortunately, although the MAHA report offers up only passing interest in Medicaid and CHIP, the Administration’s actions speak far louder. Through the passage of H.R. 1 (OBBB), President Trump has supported over $900 billion in cuts to Medicaid and CHIP, which is estimated to cut 10 million people off of coverage.
These cuts will be devastating to pediatric coverage and care. They come alongside a massive expansion of red tape, bureaucracy, and administrative barriers, such as burdensome re-enrollment requirements, confusing documentation demands, and tightened eligibility reviews.
These policies will result in millions of children losing coverage, not because they are ineligible, but because their parents missed a notice, couldn’t upload a document, or didn’t navigate the newly imposed bureaucratic system quickly enough.
This is not “reform”, and it makes nobody healthier. It’s sabotage by complexity. Technology can be used for good or it can be used to impose a bureaucracy that discourages enrollment and suppresses participation: a quiet gutting of the safety net under the guise of accountability. That will be President Trump and Secretary Kennedy’s legacy with OBBB.
And it stands in direct contrast to what a genuine child health agenda would do.
A real child health framework would provide for enrollment simplification, continuous eligibility, investing in the pediatric workforce, expanding access to mental health care, and addressing the structural determinants of child health.
In a joint document laying out some principles of importance to child health several years ago, the American Academy of Pediatrics, the Children’s Defense Fund, the Children’s Dental Project, the Children’s Hospital Association, Family Voices, First Focus Campaign for Children, Georgetown Center for Children and Families, the March of Dimes, and the National Association of Pediatric Nurse Practitioners wrote:
As a nation, we must build on what is working for millions of children, pregnant women and their families by keeping Medicaid and CHIP strong and enrolling all eligible children, strengthening private coverage, and working toward a health care system that meets the needs of ALL children, pregnant women, and their families, regardless of their health or immigration status, family income, or zip code.
Any change to our health care system must further improve coverage for children and pregnant women. They must not lose ground.
Put simply, first, do no harm.
The principles include the following standards:
All children must have health coverage that provides all medically necessary, age-appropriate benefits to promote healthy child development, and all pregnant women must have coverage for maternity and newborn care.
All children and pregnant women must have access to health care that is affordable for their families.
All children must have timely access without administrative barriers to the full range of age-appropriate health care providers, including pediatric and perinatal specialists, sub-specialists, and facilities.
All children and pregnant women must receive high quality care informed by robust [pediatric-specific and maternity] quality measurement.
All children and pregnant women must have continuous, consistent coverage with no gaps in care.
What’s missing from the MAHA strategy is any strategy to address and improve these critically important issues.
The report also lacks moral clarity. There is no commitment to health equity – no mention of the racial and geographic disparities that define the health experiences of so many children. No recognition that a child’s ZIP code still predicts their life expectancy, or that structural racism continues to shape access and outcomes. Instead, H.R. 1, the Administration’s One Big, Breautiful Bill (OBBB) is slashing health care coverage to an estimated 10 million.
Consequently, the MAHA strategy offers a technocratic word salad, empty of investment and stripped of compassion, care, and coverage.
This is more than a policy disagreement. It is a tragic failure of vision and of responsibility.
Distrust in Disguise: How the MAHA Plan Weaponizes Fear
Parents today are justifiably worried about:
Rising rates of anxiety and depression in kids
Chronic illness and asthma
Learning loss, screen addiction, and ultra-processed food
The sense that something in our systems – health, education, even childhood itself – is broken
But rather than offering a serious response to these concerns, the federal MAHA strategy feeds them into an ideological machine: one that directs attention away from structural reform and toward suspicion, blame, and disinformation.
Throughout the report, there is a consistent drumbeat that doctors are too quick to medicate, mental health diagnoses are suspect, vaccines may be unsafe, science is captured, and parents should reclaim total authority over children’s health decisions. It’s a story that flatters anxiety and reinforces distrust, while simultaneously offering few solutions that hold up under scrutiny.
Meanwhile, does the report improve health coverage of mental health services in Medicaid? Reverse the decision to block children’s mental health funding that Congress had appropriated? Address problems caused by some “parental rights” laws in states like Idaho, Texas, and Florida that create barriers for adolescents to get suicide hotline prevention counseling or mental and behavioral health care services? Improve mental health care services to foster kids who have been abused or neglected? Increase funding for community mental health services? Integrate infant and early childhood mental health care into Medicaid and CHIP?
The answer to all of these questions is NO.
Whether it is accessing health care services, getting their child immunized, or buying healthy and pesticide-free food, what the MAHA strategy encourages is the atomization and isolation of parents and children. It leaves each family to carry the burden of navigating complex, high-stakes health decisions alone, without trust in experts, without institutions to rely on, and without the assurance that the system is designed to help. It reduces health care to a series of personal gambles based on internet searches rather than a collective responsibility based on facts, science, and results.
This is not empowerment. It is abandonment.
The vast majority of parents don’t see their pediatricians, nurses, school counselors, athletic trainers, teachers, and coaches as adversaries – they see them as partners to help them with the health, education, safety, and well-being of their children.
The report questions mental health services without acknowledging the well-documented shortage of pediatric mental health providers, the increased stressors of poverty, racism, and trauma, or the fact that many children are also routinely underdiagnosed and undertreated.
It implies that doctors are eager to push unnecessary treatments, but it never acknowledges that we have a health care insurance system that imposes barriers for many families seeking to get appointments, find specialists, navigate limited insurance provider networks, or getting past prior authorization requirements and care denials. The Secretary gestures toward “root cause” solutions, but sidesteps any serious investment in community health workers, school-based health care, or family-centered care. Even worse, it completely fails to acknowledge that young people have a role to play in making decisions about their bodies, their health, and their lives.
As for immunizations, the MAHA report ignores the reality that vaccines are one of the greatest public health achievements in human history.
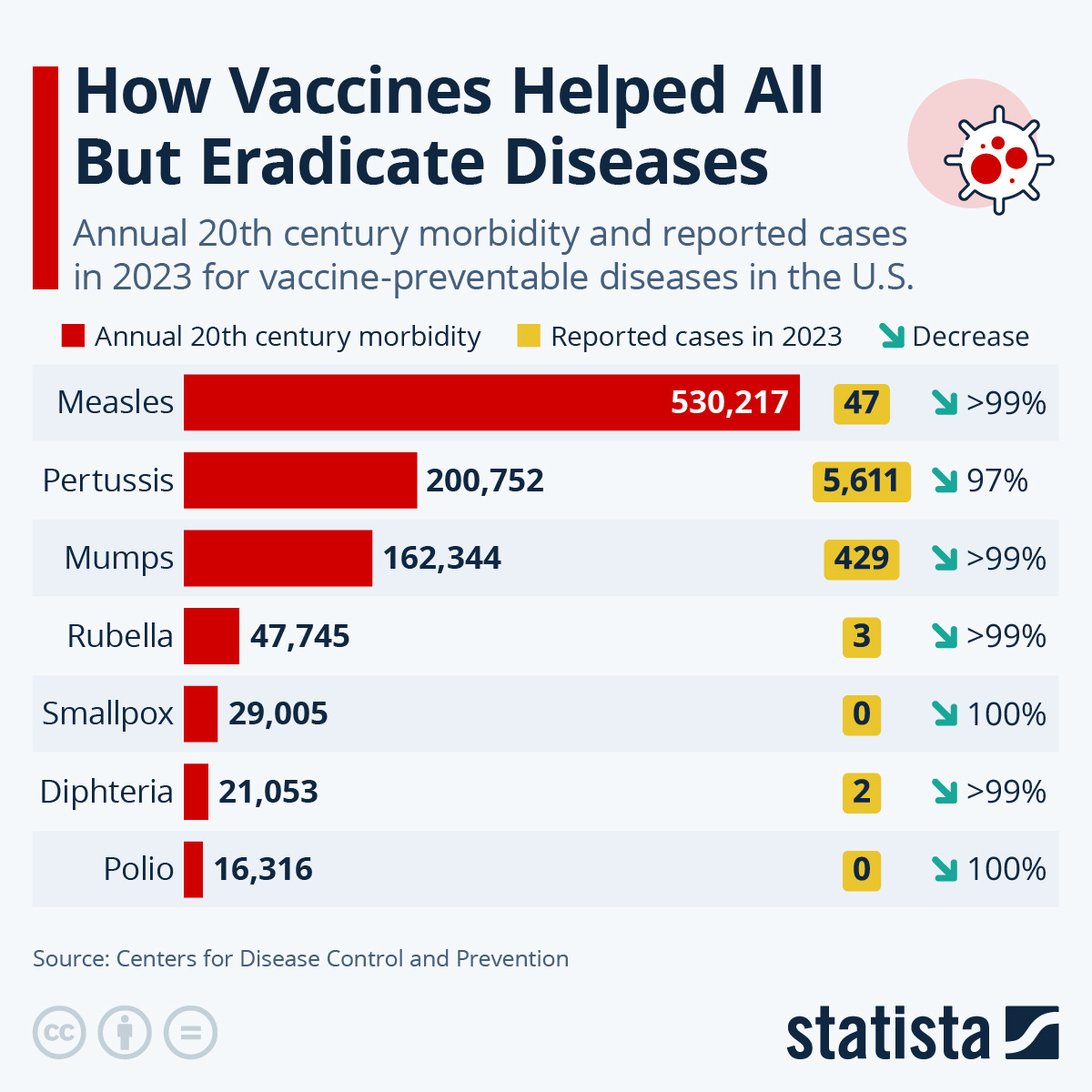
Instead, it frames immunization policy as a point of government overreach and potential harm. By highlighting “vaccine injury” and “informed consent” more than the science of disease prevention, the report gives cover to anti-vaccine narratives that have already led to falling immunization rates and rising outbreaks of preventable illnesses, such as measles and whooping cough or pertussis.
Sen. Bill Cassidy (R-LA), a physician and chairman of the Senate Health, Education, Labor, and Pensions (HELP) Committee, had some thoughts…


The MAHA report repeatedly puts forth language of distrust dressed up as reform.
President John F. Kennedy provided a far better vision back in 1962 (63 years ago!) at the signing of the Vaccine Assistance Act when he said:
There is no longer any reason why American children should suffer from polio, diphtheria, whooping cough, or tetanus – diseases which can cause death or serious consequences throughout a lifetime, which can be prevented, but which still prevail in too many cases.
I am asking the American people to join in a nationwide vaccination program to stamp out these four diseases, encouraging all communities to immunize our children and adults, keep them immunized, and plan for the routine immunization of children yet to be born.
This statement speaks to a vision of child health that centers children, treats parental concern with seriousness, but would also encourage respect for evidence, research, and clinical expertise.
We should never leave children and families to fend for themselves in an information vacuum. We advocate for restoring trust – in science, in public institutions, and in each other. Secretary Kennedy is destroying America’s leadership in medical research and science when we should be investing in more research, science, cures, and leadership.

Source: Mahler, Jonathan (2025, Sept. 15). Trump is Shutting Down the War on Cancer. New York Times.
Children and their parents don’t need scapegoats to blame. They need services that work, systems they can trust, and partners to help them achieve what’s best for them – not leaders who confuse politics with science.
Rhetoric vs. Reality – When Policy Language Betrays Children’s Health
The MAHA strategy also gives the impression of caring deeply about the environment in which children grow up. It names air and water quality, microplastics, endocrine disruptors, and pesticides. It speaks of nutrition reform, breastfeeding promotion, and the dangers of ultra-processed foods. On the surface, it sounds like a child health advocate’s wish list.
But the deeper truth is this: language isn’t leadership and the Administration’s actions directly contradict its words.
Take environmental health. While the MAHA strategy highlights chemical exposure and clean water as urgent child health issues, this Administration has moved aggressively to weaken the very Environmental Protection Agency (EPA) protections designed to safeguard those things. It has fast-tracked regulatory rollbacks, watered down enforcement, and undermined standards on PFAS (“forever chemicals”), air pollution, and pesticide use.
You cannot say you are protecting children from toxic exposure while gutting the EPA’s authority to regulate pollutants.
George Kimbrall, legal director for the Center for Food Safety, points out:
The MAHA Commission was charged with addressing the childhood chronic disease crisis. Its first report admitted pesticides were a major driver of that crisis. But when the time came to act, it turned its back on the science, the law, and the public.
Instead of proposing stronger protections, it recommended a public relations campaign, partnering with the pesticide industry, to reassure Americans that government oversight is “robust.” Instead of reining in pesticide overuse, it promises to speed up approvals. Instead of challenging the forces driving chronic disease, it has capitulated to them.
And while the MAHA report raises concerns about nutrition, it offers a vision of reform that leans heavily on individual choice and ideological purity rather than structural support. It speaks of “real food” and “nutritional integrity,” but avoids any serious commitment to:
Expanding access to WIC or school meals
Addressing food insecurity and poverty
Supporting the Child Tax Credit, which has been shown to reduce food hardship among children
Tackling food deserts, where low-income families have no access to fresh food
Instead, the report ignores that the Administration will be implementing nearly $200 billion in cuts to the Supplemental Nutrition Assistance Program (SNAP) with major ramifications for reducing access to school and summer meals for children. The report also doubles down and leans toward restricting food access in SNAP by calling for stricter definitions of “healthy” and “ultra-processed” foods. But restricting and punishing poor families for what’s in their grocery cart (“no birthday cake for your child!”) is not a public health strategy. It’s a political posture that heaps moral judgment on low-income parents without offering the means and supports to change their circumstances and access to healthy food. Furthermore, it punishes children for the status of their parents.
As Sen. Robert F. Kennedy said in Senate floor debate on June 22, 1965:
No one chooses his mother or his father, so children should not be punished because their fathers or mothers are not leading the kind of life that some Members of the Senate think they should lead.
This imposition of judgment and deservingness on parents is highlighted in the contrast of President Trump and Secretary Kennedy’s celebrate Coca-Cola’s addition of “pure cane sugar” to its beverage line-up as some sort of victory, while simultaneously deciding to impose heavy cuts to food assistance to families who rely on SNAP to feed their kids.
Neither policy change improves the health or nutrition of children.
This kind of policy-making – focused on control rather than support – mirrors broader efforts to reframe child health as a matter of personal virtue rather than public investment. It ignores the upstream drivers of poor nutrition: corporate food systems, poverty, lack of paid leave, inaccessible breastfeeding support, and underfunded schools.
By contrast, a child-focused framework would call for strengthening the programs that feed kids, funding nutrition research, and ensuring every child – regardless of zip code – has access to clean air, safe water, and healthy food.
The MAHA Report Ommission of the Leading Cause of Death in Children: Gun Violence
Perhaps the most glaring and dangerous void in the MAHA report is this: there is not a single mention of gun violence, the leading cause of death for children and teens in America.
This omission isn’t just policy malpractice: it’s a moral failure.
According to the Johns Hopkins Center for Gun Violence Solutions, more than 2,500 children died from firearm injuries in 2022 alone. These deaths surpass those from cancer, car accidents, infectious disease, poisonings, or drownings.
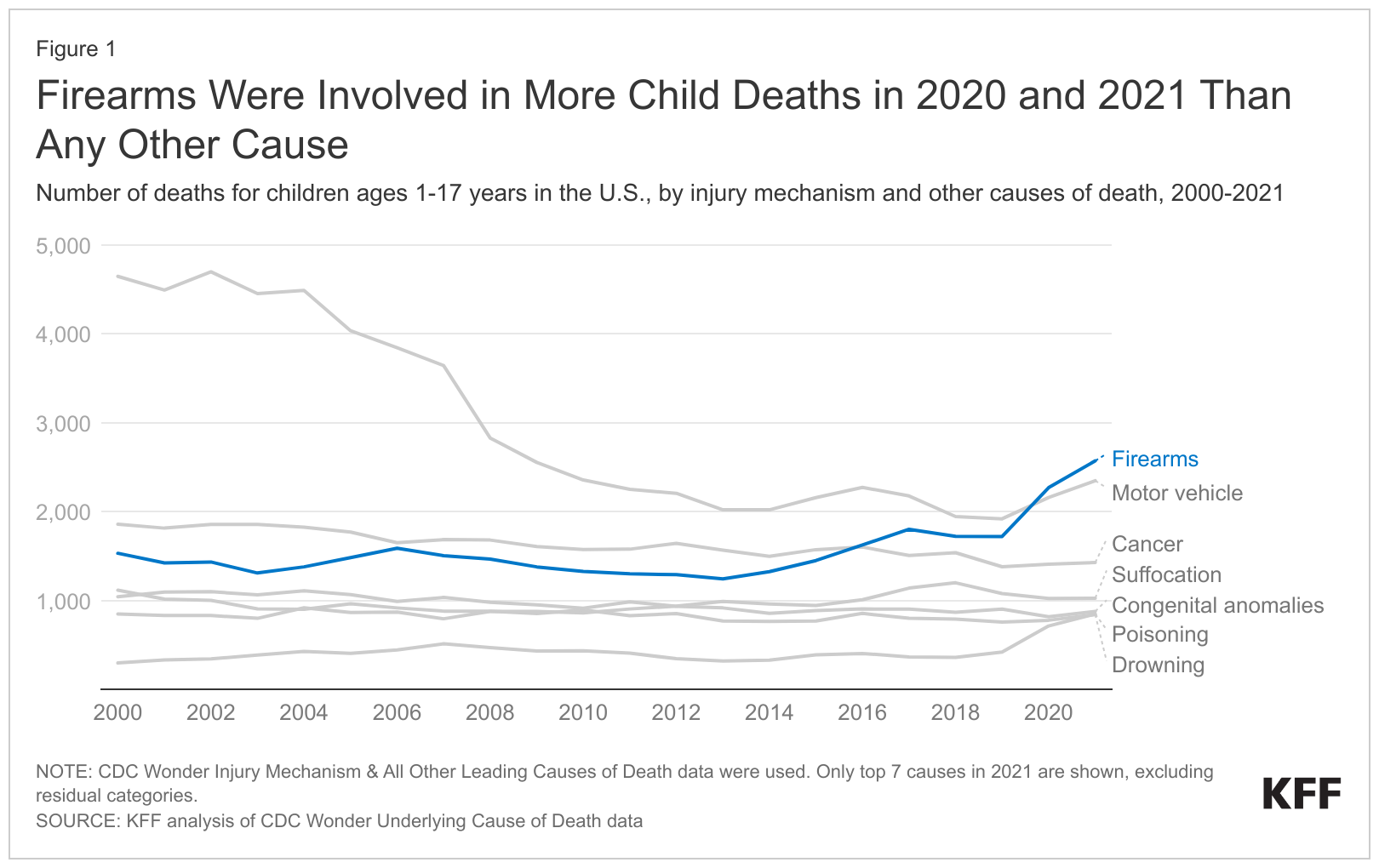
Gun violence is a daily threat to children’s health – on playgrounds, in schools, in homes, and on neighborhood streets. Pediatricians, emergency physicians, educators, and parents alike have called this crisis what it is: a public health emergency.
Yet the federal MAHA strategy is silent – not a single word. No goals. No funding. Not even acknowledgement.
As the Los Angeles Times reported this past week, RFK Jr. and his allies have repeatedly deflected when asked about firearms, blaming rising violence on antidepressants, social media, or video games instead. This rhetorical sleight-of-hand shifts attention away from gun access and onto vague cultural decay – turning a preventable epidemic into a culture scapegoat.
While the MAHA plan claims to prioritize “root causes,” it refuses to address the root cause that is literally killing our kids.
In fact, there is no mention of:
Safe storage laws
Gun violence prevention programs
Research on firearm injury
Support for trauma-informed care
Community violence intervention
Background checks
Restrictions on assault weapons
Red flag laws
These are not partisan demands. They are life-saving interventions.
You simply cannot claim to care about children's health while ignoring the number one killer of children.
If HHS truly wishes to champion child health, it must be held accountable for what it chooses to ignore. Silence in the face of violence is not neutrality. It's complicity.
Undermining Trust, Abandoning Responsibility
Beneath the MAHA strategy’s glossy exterior lies a corrosive message: don’t trust the system. Not the doctors. Not the scientists. Not the public health agencies. Not the institutions that have protected generations of children from disease, disability, and death.
Throughout the report, this distrust is dressed up in the language of “freedom,” “transparency,” and “conflict of interest.” It suggests that science can’t be trusted unless it’s stripped from the institutions that created it, and that parents must navigate health decisions with little more than instinct and internet searches.
But this is not empowerment: it’s what is called “atomization” – the breakdown of shared systems, leaving individuals isolated and unsupported in navigating complicated challenges. The strategy cuts parents and their off from the evidence, guidance, help, and collective trust that make decision-making possible in complex systems.
The clearest and most troubling example is in the report’s approach to vaccines, which overtly aligns with anti-vaccine rhetoric that has already led to declining immunization rates and the reemergence of diseases like measles and pertussis.
But the distrust doesn’t stop there. The report also calls for:
Parallel research systems, detached from established academic and federal institutions
A new “framework” for validating science, designed to question conventional peer review
Expanded focus on supplements, nutraceuticals, and alternative treatments
This last point is especially telling. The MAHA report critiques mainstream medicine for being insufficiently rigorous, and yet, promotes dietary supplements as a central pillar of child health, despite the fact that most are unregulated, unproven, and unsupported by pediatric research. While immunizations are framed as suspect, the $50 billion supplement industry is given a free pass.
This is not about freedom. It’s about fragmenting truth that, once again, leaving parents and children alone in a health information wilderness where corporate marketing and ideological pseudoscience can masquerade as expertise.
By contrast, a real child-focused framework would start from a simple but powerful premise: parents and families deserve systems they can trust. That means:
Investing in public health agencies, not undermining them
Protecting vaccine infrastructure, not destabilizing it
Funding pediatric research through respected institutions, not discrediting them
Building health literacy and cultural competency, not flooding the zone with false equivalence and disinformation
We believe in transparency and accountability too, but not as weapons against science. We believe in medical freedom too, but only when all families have real access, real information, and real support.
A Call to Remember Who We’re Fighting For: Children
“The work goes on, the cause endures, the hope still lives, and the dream shall never die.”
— Senator Edward M. Kennedy (Aug. 12, 1980)
I witnessed Sen. Kennedy’s speech when I was in high school and remember thinking that statement wasn’t just political. It was about moral obligation and a call for the nation to make progress on the fight for justice, equity, and opportunity, especially for those without power or voice. No group fits that description more than children.
The federal MAHA strategy asks us to believe that public health has failed, that expertise is corrupt, and that parents are on their own. But real leadership doesn’t abandon people to chaos. It builds systems they can rely on. It brings clarity where there is noise, solidarity where there is isolation, and truth where there is confusion.
If we are serious about making our children healthy again, then we must start:
With investment, not ideology
With trust in public institutions, not nostalgia for a past that never existed
With a commitment to equity, not moral judgment
That means:
Protecting and expanding Medicaid, CHIP, WIC, and school health programs
Defending vaccines and the public health infrastructure that underpins them
Funding pediatric research and mental health with seriousness and stability
Addressing the environmental and economic conditions that shape children’s lives before they ever step into a clinic
Centering racial, geographic, and disability equity in every policy decision
Child health policy should make children the focus and priority. Unfortunately, in Secretary Kennedy’s MAHA report, children are being pushed to the margins of policymaking – once again.
As President John F. Kennedy told the nation in a Valentine’s Day message in 1963:
The future promise of any nation can be directly measured by the present prospects of its youth.
Measured by that standard, the MAHA strategy fails. But we still have time and the tools to write a different future.
It’s time to choose science over cynicism, community over isolation, and investment over rhetoric. Let’s choose children: not just in words, but in actions.
The Kennedys of past generations understood this. It’s unclear whether Secretary Kennedy will – before it’s too late.

What You Can Do:
Subscribe to Kids Can’t Wait (and please consider being a paid subscriber) because kids can’t vote, but with your support, we can help advocate for them.
Join us as an Ambassador for Children to speak up for our nation’s children.
Call your federal and state legislators to support a REAL agenda to improve child health, safety, and well-being.