



Stop Threatening the Health of Children

Child well-being is important for the future of our country. When we ensure the healthy growth and development of the next generation, they will pay that back through education achievement, economic productivity, and responsible citizenship. It is in all of our interest that politicians and bureaucrats should not threaten or gamble with the health of our nation’s children.
And yet, far too many do.
Prior to the consideration of “repeal and replace” bills for the Affordable Care Act (ACA), children’s groups made the request that policymakers adopt a “do no harm to children” standard. It was a pretty simple and fundamental request.

This was because, at the beginning of 2017, child advocates were facing a triple-threat to the health of children, which included:
Threats to children due to the proposals to repeal the ACA, which would have eliminated coverage to children enrolled in the marketplaces and gutted important consumer protections, such as the ban on pre-existing conditions exclusions, annual and lifetime limits, and benefit requirements;
Threats to children caused by the proposals in the House and Senate to slash Medicaid by between $700–870 billion over 10 years through either block grants or per capita caps, which are arbitrary limits that would be imposed on funding for health coverage; and,
Threats to the Children’s Health Insurance Program (CHIP), which was set to expire in September 2017.
These dangers to the health and well-being of children in all three policy areas stretched the capacity of an already strained and limited child advocacy community. For example, while most health advocates were focused on the proposals to repeal the ACA and slash Medicaid funding, children’s organizations were working on those issues and simultaneously pushing for the reauthorization of CHIP.
Child advocates were rightly concerned that, although everybody covered by Medicaid would be hurt by cuts to the program, kids would likely be disproportionately harmed. In fact, throughout 2017, those initial fears were to be confirmed repeatedly.
In fact, as Congress sought to impose arbitrary limits upon the Medicaid program through either block grants or per capita caps, the Congressional Budget Office (CBO) confirmed that states would be forced to make choices about how to meet the arbitrary caps or limits. As federal policymakers were looking to hit certain budget savings from Medicaid cuts, children were frequently targeted.

For example, the House proposed to impose block grants upon children but not on senior citizens or people with disabilities. Moreover, the Senate proposed per capita caps that would have disproportionately negatively impacted the allowable inflation rate allowed by the legislation.
Simultaneously, while Congress was spending the first three-quarters 2017 on these bills before the Senate bill’s failure by just one vote in the wee hours of the morning on July 28, 2017, and the Graham-Cassidy effort also died in late September, child advocates also had to simultaneously push, with little success, for the reauthorization of CHIP. Sadly, despite bipartisan agreement on the framework for reauthorization of CHIP, partisan disagreement on “pay-fors” and partisan “hostage taking” of the politically popular program to further other political agendas related to the budget and immigration fights left CHIP in limbo for more than four months.
These are things we knew and were public, but newly released correspondence between Centers for Medicare & Medicaid Services (CMS) Administrator Seema Verma and Dennis Smith, Senior Advisor for Medicaid & Healthcare Reform for the Arkansas Department of Human Services confirm even deeper threats to the health coverage for children within these important federal and state departments.
These documents came to light because American Oversight filed a Freedom of Information Act (FOIA) request on August 17, 2017, for correspondence between Administrator Verma and Smith to review whether Verma had violated ethics requirements that precluded her working on matters involving states she previously worked for as a consultant.
Ouf of the 77 pages of released documents, child advocates should be fully aware of and concerned about a number of the issues that were raised and discussed by Verma and Smith related to children’s health coverage, including some information about the Medicaid work requirements waiver that CMS granted Arkansas and has led to the disturbing loss of Medicaid coverage for thousands of people.
Furthermore, in a document entitled “The Rubik’s Cube of the American Health Insurance System” that was passed between the two agencies, the paper supports repealing the ACA and the marketplaces, in part, because “[t]here is no national health insurance market.”
Unfortunately, prior to the creation of the ACA marketplaces, the non-employer, individual insurance marketplace was a disaster. The individual market created an enormous barrier to coverage for millions of children and families, including the lack of affordable options, medical underwriting, restrictions on coverage for people with pre-existing conditions, and the imposition of annual and lifetime limits.
The Rubik’s Cube paper argues for using children as a pawn by moving children covered by Medicaid and CHIP into the individual market so as to prop up that market for more older, less healthy, and more expensive populations. Despite the glaring fact that the proposal would leave millions of low-income children worse off in terms of benefits, affordability, and provider networks, the paper attempts to justify such a move by arguing:
There are numerous examples of other industries that attract people of all income levels and age groups by offering a wide array of choices. Millions of the young, healthy lives needed to stabilize premiums in the individual market are ensconced in the Medicaid and CHIP programs. If the benefits and subsidies in the individual market are not sufficient to make coverage in the individual market attractive, then people will stay on Medicaid. . . That is a rational decision for an individual or family to make, so the flaw is in the design which makes one program more attractive than another.
First, children should never be treated as pawns to further some other political or ideological agenda. And yes, wanting to protect and stay on Medicaid is absolutely rationale. Let’s be clear, Medicaid and CHIP are not a “flaw in the design.” They are “more attractive” because they work and are far better coverage for children than the individual market.
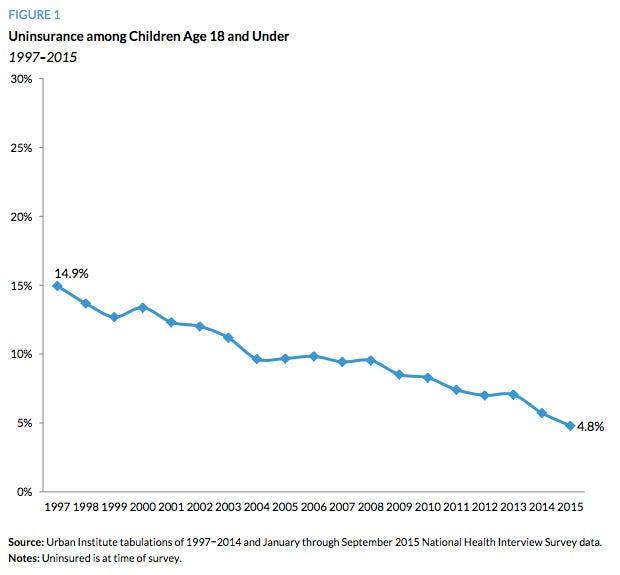
In fact, Medicaid and CHIP have, in tandem, successfully slashed the uninsured rate for children from around 15 percent in 1997 to less than 5 percent today. For millions of children, the passage of CHIP in 1997, which Smith and I worked on together in the Senate, has proven to be a bipartisan success story.
To address this so-called “flaw” (which again, is comprehensive, affordable, pediatric-focused coverage), the idea would be to move the non-elderly and non-disabled adults and children currently served by Medicaid and CHIP with income above 100% of poverty into the non-group or individual market. The vast majority of those negatively impacted by such a proposal would have been children.
The logic is shocking.
If a school has one really good engineering teacher and another that is awful so nobody wants to take his or her class, the solution is not to fire the good teacher to help fill the class of the bad teacher, but that is exactly what this proposal would do. To help either the bad insurance product or the bad teacher, every single child would be sacrificed and left worse off.
Again, first, do no harm.
The FOIA documents also confirmed for child advocates that people were discussing using CHIP as a potential hostage to even move their stalled health care legislation. On March 26, 2017, Smith wrote an email to Verma uring her to cheer up (“the sun came up this morning”) and that there were other options to move the legislation forward, such as reducing the amount of Medicaid savings that the House was seeking. He also wrote:
there are still levers to be pulled — SCHIP [sic] reauthorization and deficit reduction
Fortunately, Congress rejected using CHIP as a hostage in the health reform debate. On the other hand, both parties sought to use CHIP as a way to try and pass either a budget or immigration bill.

The FOIA request also confirmed that children were targeted to absorb a disproportionate level of cuts from the Medicaid caps.
Frankly, children do not vote and do not have political action committees (PACs) that can lobby for their interests. Consequently, it is not surprising that Smith wrote to Verma on July 21, 2017, to urge greater protections for senior citizens and people with disabilities than for children. He explained:
As you know, Gov. [Asa] Hutchinson [R-AR] remains concerned about including disabled and elderly under the per capita caps. therefore, have drafted to cover children and adults. hope that is helpful.
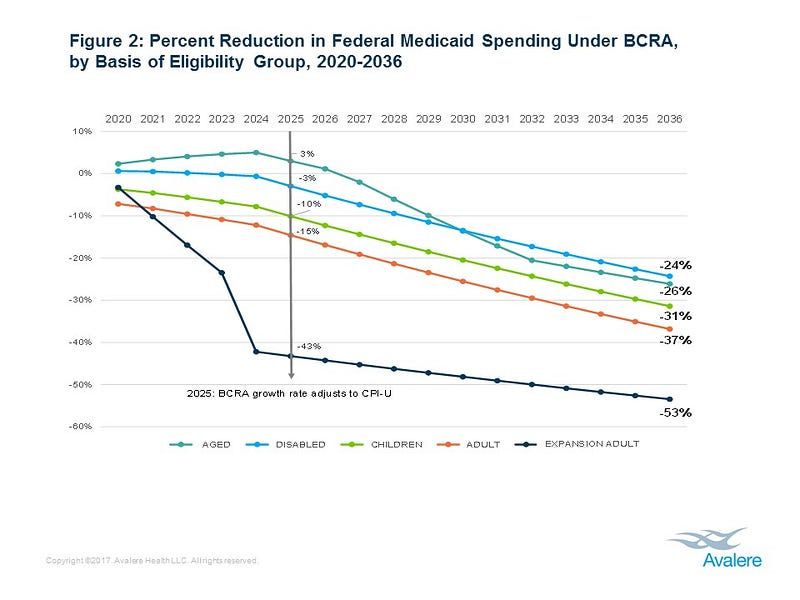
Although Smith and the Arkansas governor did not get what they wanted, per se, because senior citizens and people with disabilities were included in the per capita cap, the cap was set to disproportionately harm children.
In fact, it got worse for children as the process continued. As federal lawmakers sought to obtain a certain level of savings in Medicaid, their efforts to lessen the harm to senior citizens and people with disabilities led to a growing gap between the harm it would have on senior citizens and people with disabilities compared to children and non-disabled adults. These two charts by Avalere Health highlight these changes as the process moved forward.

Fortunately, the Senate legislation was rejected and CHIP was finally reauthorized months after its expiration, but the threats to child health remain unabated. As examples:
Just days after CHIP’s reauthorization, the President proposed a $15 billion rescission package that included $7 billion in cuts to CHIP that also only failed by just a single vote in the Senate.
Although CHIP was reauthorized by 10 years, the legislation includes a “cliff” in the final year that will potentially create an enormous funding shortfall when it comes up for reauthorization again in 2026, which is something no other federal health program (e.g., Medicare, veterans health, the Federal Employees Health Benefits Program, etc.) is subjected to.
There is a lawsuit filed by a subset of state Attorneys General and supported by Attorney General Jeff Sessions that would gut pre-existing conditions protections, annual and lifetime caps, and other important consumer protections for children and families.
CMS is soliciting Medicaid waivers from states on issues like work requirements that have already had negative impacts on the coverage of adults, including the parents of children. Although there may be the expectation that does not harm children, it does (as is highlighted in this comment letter to South Dakota’s waiver request).
The Administration is considering a “public charge” rule that would undermine the Medicaid coverage of legal immigrants and their children and that might also negatively impact CHIP coverage.
The Environmental Protection Agency (EPA) has placed Ruth Etzel, the pediatrician leading the Office of Children’s Health Protection, on leave as an apparent move to minimize or eliminate the office in charge of protecting children’s health — an office that former Bush EPA Administrator Christine Todd Whitman described as “critical to the health of the future.”
We would, once again, urge policymakers to “first, do no harm” to children’s health. We have made enormous strides in this country to successfully cut the uninsured rate by two-thirds since the passage of CHIP in 1997. Rather than considering policy proposals that would clearly disrupt and harm children’s health coverage, policymakers should simply ask themselves and affirmatively answer the question, “Is it good for the children?”

The health of children is the future power of our nation. If our children aren’t healthy, they aren’t going to learn, and we aren’t going to remain as the world’s leader in innovation and technology in the future.
We should be investing in kids and not gambling with our children’s health. Medicaid and CHIP are working for our children. As Texans like to say, “If it ain’t broke, don’t fix it.”
Lawmakers should not undermine the coverage of millions of children that rely on that coverage. It is critical that children should never be treated as pawns and their health be put at risk in order to further other political agendas.
There is a better path.
Instead of considering proposals that would take health coverage of children backward, we should all be working together to improve the health of our kids. We should be working to reduce infant and maternal mortality, improving access to care, improving health care quality, and expanding cost-effective prevention efforts.
If Congress wants to make cuts, it should start with programs that don’t work — not the ones that protect Americans like Medicare, Medicaid, and CHIP.
*****
If you would like to help ensure that children and their needs, concerns, and best interests are no longer ignored by policymakers and to protect our nation’s public schools from continued assault, please consider joining us as an “Ambassador for Children” or becoming a paid subscriber to help us continue our work on behalf of children.